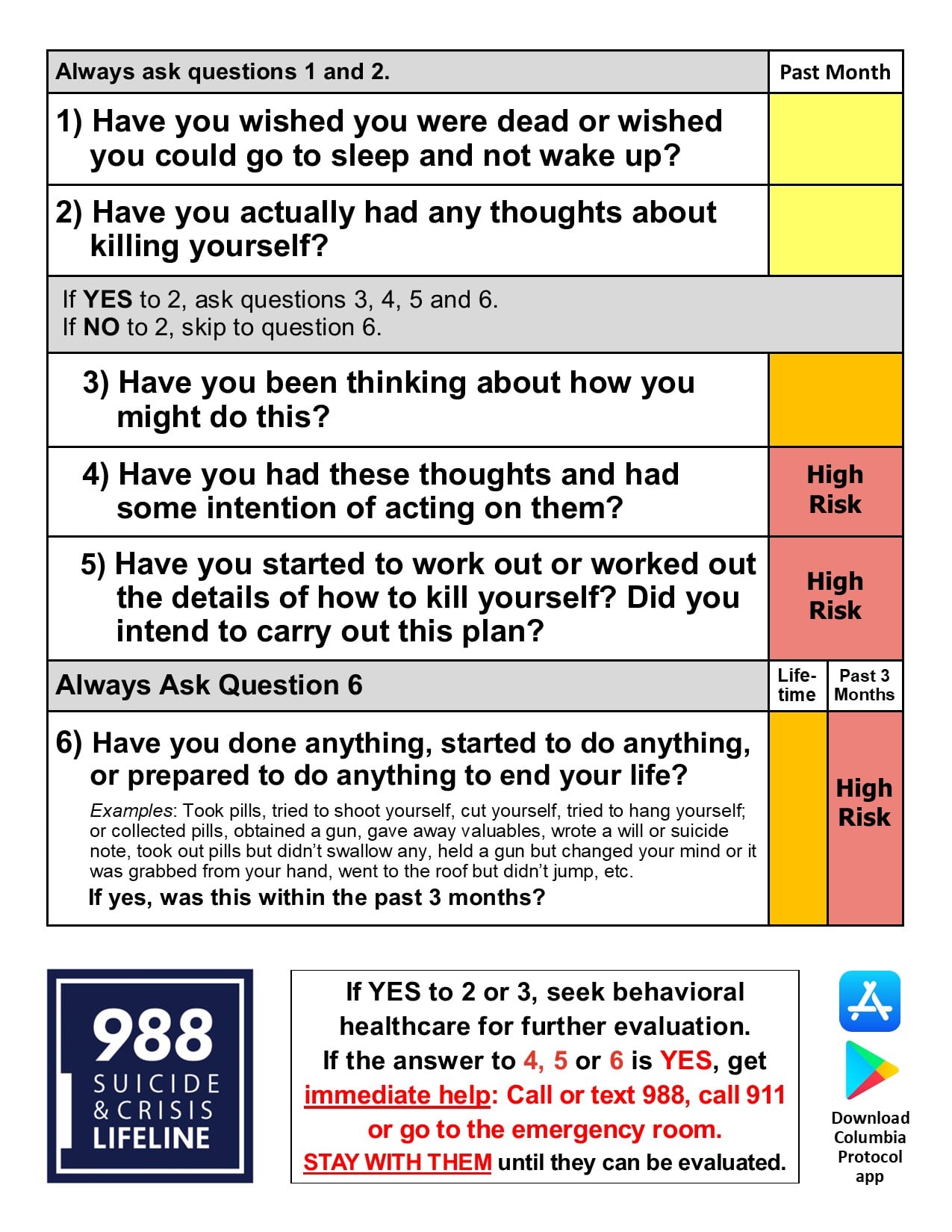
The Columbia Protocol, also known as the Columbia-Suicide Severity Rating Scale (C-SSRS), supports suicide risk screening through a series of simple, plain-language questions that anyone can ask. The answers help users identify whether someone is at risk for suicide, determine the severity and immediacy of that risk, and gauge the level of support that the person needs. Users of the tool ask people:
Protocol administrators ask a series of questions about suicidal thoughts and behaviors. The number and choice of questions they ask depend on each person’s answers. The questioner marks “yes” or “no,” as well as how recently the thought or behavior occurred and a scoring of its severity. The shortest screeners are condensed to a minimum of two and a maximum of six questions, depending on the answers, to most quickly and simply identify whether a person is at risk and needs assistance. For a more thorough risk screening, Columbia Protocol askers should use the standard scale.
The Columbia Protocol questions use plain and direct language, which is most effective in eliciting honest and clear responses. For example, the questioner may ask:
To use the Columbia Protocol most effectively and efficiently, an organization can establish criteria or thresholds that determine what to do next for each person screened. Decisions about hospitalization, counseling, referrals, and other actions are informed by the “yes” or “no” answers and other factors, such as the recency of suicidal thoughts and behaviors.
The Columbia Lighthouse Project provides many examples of triage documents that Columbia Protocol users in hospitals, primary care practices, behavioral health care facilities, military services, prisons, and other settings employ to make these decisions. The Project also provides assistance to any organization that is thinking through its policy and establishing a care plan.





The first step in effective suicide prevention is to identify everyone who needs help. The Columbia Protocol was the first scale to address the full range of suicidal thoughts and behaviors that point to heightened risk. That means it identifies risk not only if someone has previously attempted suicide, but also if he or she has considered suicide, prepared for an attempt (for example, buying a gun, collecting pills, or writing a suicide note), or aborted plans for suicide because of a last-minute change of mind or someone’s intervention.
The Columbia Protocol screens for this wide range of risk factors without becoming unwieldy or overwhelming, because it includes the most essential, evidence-supported questions required for a thorough screening. The Columbia Protocol is:
Columbia University, the University of Pennsylvania, and the University of Pittsburgh — supported by the National Institute of Mental Health (NIMH) — developed the screening tool for a 2007 NIMH study of treatments to decrease suicide risk among adolescents with depression. The Columbia Protocol, based on more than 20 years of scientific study, filled an urgent need for suicide research and prevention: a better way to uniformly and reliably identify people who are at risk. The Columbia Protocol achieved accurate and comparable results by using consistent, well-defined, and science-based terminology. Just as important as its ability to identify who might attempt suicide, it was the first tool to identify the full range of a person’s suicidal ideation and behavior, including intensity, frequency, and changes over time. .
In 2011, the Centers for Disease Control and Prevention adopted the protocol’s definitions for suicidal behavior and recommended the use of the Columbia Protocol for data collection. In 2012, the Food and Drug Administration declared the Columbia Protocol the standard for measuring suicidal ideation and behavior in clinical trials. Today, the Columbia Protocol is used in clinical trials, public settings, and everyday situations, such as in schools, faith communities, hospitals, and the military, to identify who needs help — saving lives in 45 nations on six continents.
“It’s about saving lives and directing limited resources to the people who actually need them. ”
Dr. Kelly Posner Gerstenhaber, Founder and Director, The Columbia Lighthouse Project